How Randomized Control Trials are revolutionizing the fight against poverty?
Randomized Control Trials (RCTs) have transformed the world of developmental economics and redefined how policy-makers view and tackle the problem of extreme poverty. By providing robust evidence on what works and what doesn't, RCTs have enabled a more scientific approach to policy decision-making, shifting from ideology and assumptions to data-driven and evidence-based policies. But what exactly are Randomized Control Trials? And more crucially, why have they emerged as the most potent tools in our fight against extreme poverty?

648 million people live in extreme poverty, earning less than 2.15 USD per day. That means not having access to basic education, healthcare, housing, and struggling for even two meals a day.
The Thankful Poor by Henry Ossawa Tanner, 1894.

That's almost twice the number of people living in the United States of America.
That's a shame! As Amartya Sen famously said, "Poverty is not just a lack of money; it is not having the capability to realize one's full potential as a human being."
Portrait of Amartya Sen. © Nobel Foundation archive
However, extreme poverty rates have been rapidly falling. In 1990, more than a third of the global population lived in extreme poverty. Today it is less than one-tenth.
42% of the global population lived in extreme poverty in 1989.
9% of the global population lived in extreme poverty in 2019.
WHAT IS THE REASON FOR THIS DECLINE?
Economists have long pointed to the industrialization of nations as the key driver which can lift people out of poverty and give them a better quality of life.
Maschinenbau-Anstalt Borsig, Berlin Chausseestraße by Karl Eduard Biermann, 1847.
China indeed proves this hypothesis. In 1981, almost the entire population in China was living below the International Poverty Line (IPL). But as the economy grew at an exponential pace, the share of people below the IPL became almost negligible.
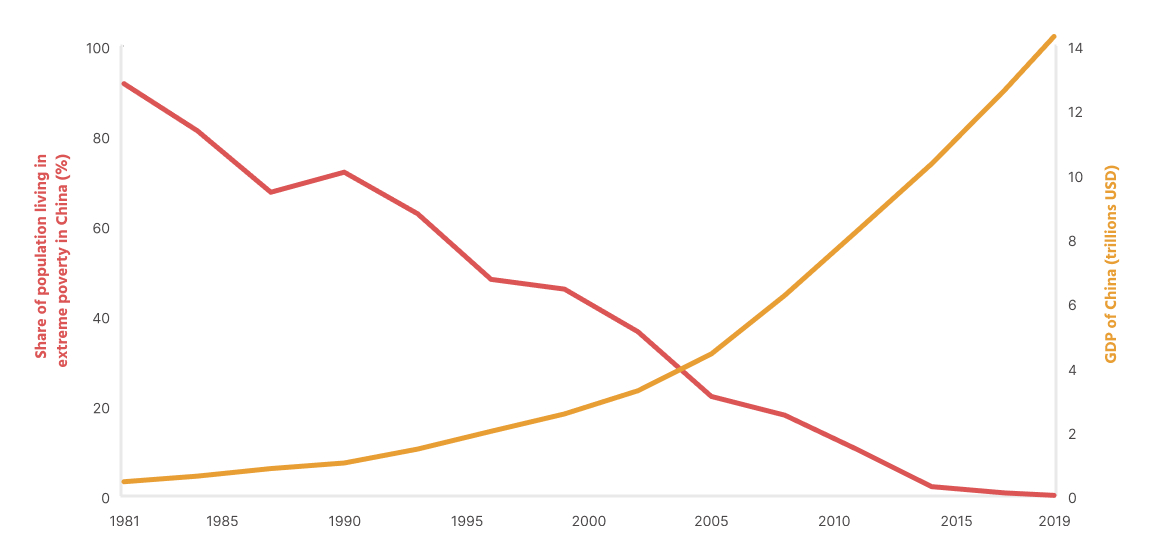
The challenge with relying on Development as the answer to helping people caught in the cycle of poverty is that it takes decades for a nation to industrialize, and we can't be sure what worked in China will work elsewhere.
The more urgent question is: what can be done in the present?

Governments around the world have long relied on social welfare policies as a major tool in the fight against poverty.
The Meaning of Social Security by Ben Shahn, 1946

Some examples include free school lunches in India, Food stamps in the USA, The right to 100 days of employment for every adult in India and Rationed food for the people who fall under the poverty line.
© Getty images
However, some economists and policy-makers argue that there is no direct evidence that these programs are effective at solving the problems they are designed for. While observational studies have shown that these programs have a positive impact, they are often criticized for their inability to establish causality. In an observational study, we cannot control for all possible confounding factors, and the observed associations may have been influenced by unmeasured or unobserved variables. That is, we cannot prove beyond a reasonable doubt that the cause (intervention in the form of welfare) produced the effect (positive impact on the lives of the poor).
Decades ago, this was the same problem facing the medical community. Researchers couldn't conclusively say whether the outcome of a treatment was the result of the treatment itself or some other unmeasured or unobserved variable.

The search for cause and effect is hundred of years old. Philosophers and scientists have been pondering this question for millennia. How can we be sure that the cause is what produced the effect?
Interior of the Laboratory of the Apothecary Stoockhuys by Johannes Jelgerhuis, 1818.

Till the nineteenth century, bloodletting was (drawing out a person's blood using surgical methods) thought of as a fantastic cure for most ailments.
Breathing a Vein, a caricature of bloodletting by venesection by James Gillray, 1804.

When George Washington developed a swollen, sore throat in 1799, he asked his overseer to bleed him. Doctors then drained nearly half his blood. He died within a day.
Life of George Washington: The Christian by Junius Brutus, 1853.
Flemish Chemist Jan Baptist van Helmont believed that evacuation (i.e. inducing vomiting and defecation) was a better approach, and he proposed a simple way to settle the argument once and for all.
Portrait of John Baptist Van Helmont, artist unknown, 1682.
Van Helmont suggested taking 200 patients with similar symptoms and dividing them into two groups by randomly allocating them to one of the groups (to remove any bias in selection). Half of the patients would be treated by Van Helmont using evacuation and the other half by the more widely used method of bloodletting.
Treatment - To be treated using Evacuation
Control - To be treated using Bloodletting
The success of the treatment can be determined by finding out the number of people who die in each group (Since the groups are fairly similar, any differences in the death rate would be because of the treatment and not some other factor). He says as much: "I will cure them without bloodletting… [and] we shall see how many Funerals both of us shall have." (Van Helmont never got to carry out his experiment)
But the idea was still not fully developed. For example, there was no untreated control group to compare the effects of our treatment. What would have happened if there was no intervention (Bloodletting or Evacuation)?
Portrait of Louis Pasteur, artist unknown.
That idea of an untreated control group came later, with the famous experiment of microbiologist Louis Pasteur who was trying to prove that he had developed an animal anthrax vaccine. To test the efficacy of his vaccine, he asked for 60 sheep and split them into three groups: Treatment Group, Untreated Control Group, and Control Group. The treatment group was exposed to the virus and given the vaccine; the untreated control group was also exposed to the virus but not given any vaccine, while a third group was neither exposed to the virus nor given the vaccine. The results were stark: all the exposed but untreated sheep died, while all the vaccinated sheep survived healthily.
So, how can Randomized Control Trials help us fight poverty?

Economists are concerned about the reliability of previously used methods for identifying causal relationships and grand theories of development.
The Moneylender and His Wife by Quentin Matsys, 1514.
Many economists today say that focus on "small" problems is more likely to succeed rather than the grand theories of Development, which excluding some outliers, have failed to solve the problem of poverty.
They argue that randomized experiments are a simple solution to causal questions and bring credibility to economic analysis.
Black chalk board with chalk writing by Mick Haupt on Unsplash

Randomized experiments in development economics have gained popularity since the early 1990s and gathered momentum in the 2000s, especially through the work of economists Abhijeet Banerjee, Esther Duflo and Michael Kremer. They were awarded the Nobel Prize in 2019 "for their experimental approach to alleviating global poverty".
Portrait of Abhijeet Banerjee, Esther Duflo, and Michael Kremer. © Nobel Foundation Archives.
In 2007, only around 44% of children aged 1-2 in India were immunized with the basic package of vaccines.

© Associated Press
Understanding how to increase the immunization rates is important not only for existing vaccines but also to maximize the uptake of any new vaccine. The economists Abhijeet Banerjee, Esther Duflo, and Rachel Glennerster set out to find what could be done.
The researchers found that parents were not immunizing their kids because the public health centres where the vaccine doses were administered were often closed or the nurses were absent. Additionally, the parents were not entirely sold on the benefits of immunization and taking their kids to the immunization centers (which were not guaranteed to be open) meant forgoing a day's wage. They believed that having a reliable supply of free immunization services and incentives to improve the demand for these services could improve immunization rates.
Abhijeet Banerjee, Esther Duflo, and Rachel Glennerster designed a Randomized Controlled Trial (RCT) study to assess the efficacy of modest non-financial incentives on immunization rates in children aged 1-3.
The Randomized Control Trial (RCT) design is important because by randomly assigning participants to receive the intervention or not, the researchers can control for other factors that may influence the outcome, such as socioeconomic status or access to healthcare. RCT allows the researchers to attribute changes in immunization rates to the interventions more confidently.

They selected rural Udaipur in Rajasthan to study on the effect of incentives on increasing immunization rates. This area had criminally low rates of immunization. Only 2% of kids had been immunized here.
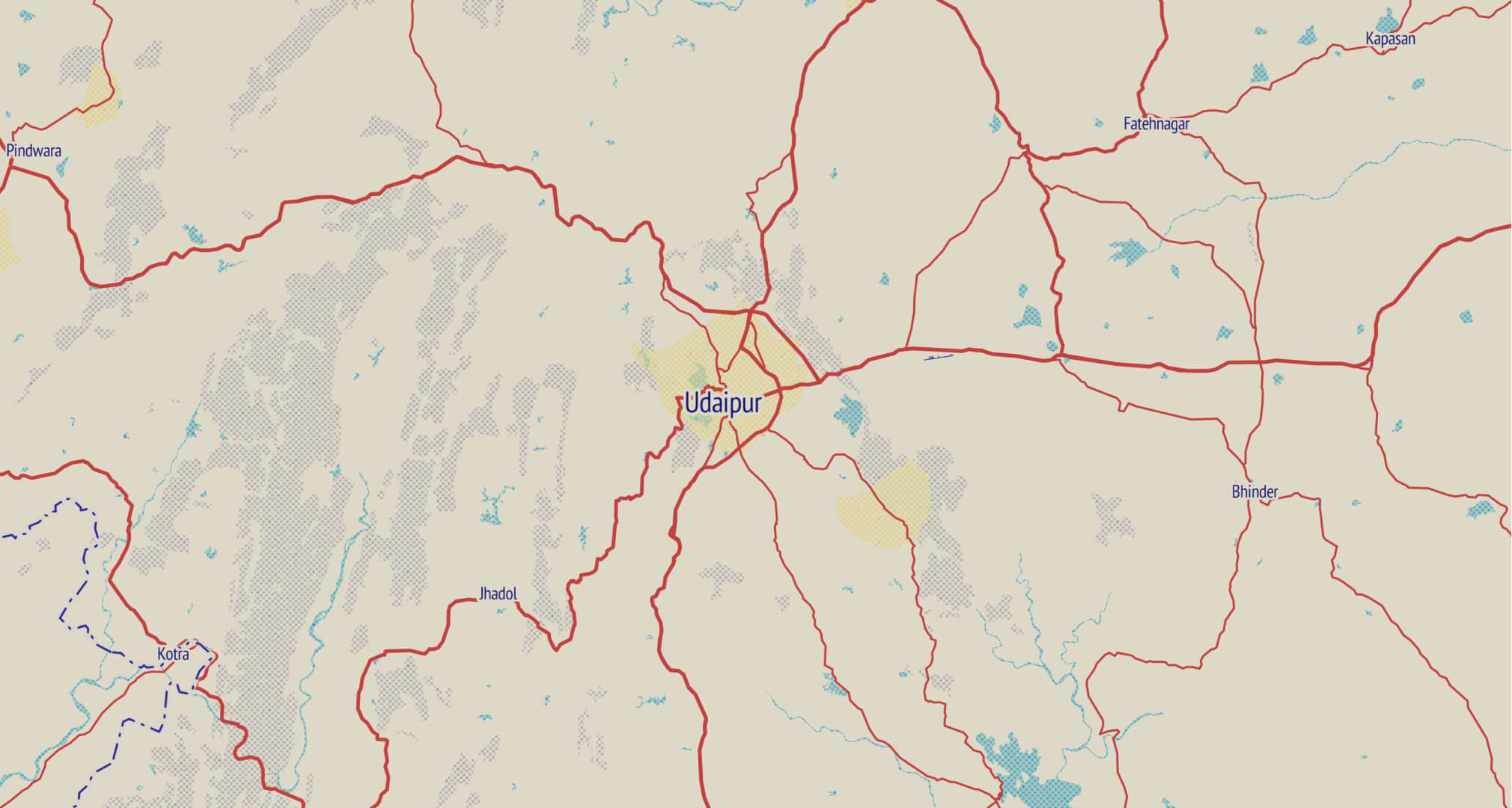
The researchers randomly selected 134 villages in and around Udaipur, Rajasthan. These villages all had poor health infrastructure and high rates of absenteeism among the health workers.
Within each village, 30 households containing children aged 0-5 years were randomly selected to be part of the study.
These villages were then randomly divided into three groups: Intervention A (30 villages), Intervention B (30 villages), and Control (74 villages).
Control 50 out of 860 children fully immunized. These children formed part of the control group and had access to the standard vaccination services but did not receive any interventions.
Control Group: 6% Fully Immunized
Intervention A 68 out of 379 children fully immunized. This group had access to regular, well-publicized clinics but did not receive any incentives for completing partial or full immunization.
Intervention A: 18% Fully Immunized
Intervention B 148 out of 382 children fully immunized. This group had access to regular, well-publicized clinics. They also received 1 kg lentils for each vaccination and a set of metal thalis for completing full immunization.
Intervention A: 18% Fully Immunized
Intervention B: 39% Fully Immunized
This study showed that offering incentives does, indeed, result in higher immunization rates. By doing a randomized control study, the authors could be sure that the increase in immunizations (effect) resulted from providing incentives (cause) and was not a result of some other unaccounted factor.
Today, Randomized Control Trials have revolutionized the field of welfare economics. Abdul Latif Jameel Poverty Action Lab (J-PAL) at the Massachusetts Institute of Technology has conducted over 800 policy experiments in around 80 countries using RCTs. The world bank also established a dedicated impact evaluation unit to conduct randomized trials, which accounts for two-thirds of all evaluations.
One such study conducted by a team of MIT and Yale researchers wanted to answer whether a "big push" approach, providing a package of assets and support to the ultra-poor, can help the extreme-poor establish sustainable self-employment activities and generate lasting improvements in their well-being.

The researchers ran a three-year "Graduation Program" in six countries, giving the poorest members of a village a choice of assets such as goats or chickens. The program also included weekly cash or food transfers, savings account access, and mentoring. Over 10,000 households were randomly assigned to receive the "Graduation" intervention.
© Getty images

Income-generating assets such as goats or chicken.

Training to use the assets to start a business, such as producing and selling milk.

Training in health, nutrition and hygiene.

Food or Cash transfers.

Access to a savings account and encouragement to save.

Regular visits from field officers to ensure accountability.
The package was designed to provide holistic support to the families.
The researchers conducted a follow-up evaluation two years after the program was initiated, and returned for another assessment a year later to evaluate the program's long-term effects. Overall, the results showed significant improvement across almost all indices that were measured.

The program also led to a doubling of the amount that people saved.
RCTs, employing the most rigorous statistical methods, challenge the criticism of some policy-makers and economists who say that social welfare programs are ineffective in the fight against poverty and are a waste of taxpayers' money. They help us design better policies that could help the poor live a dignified life, whether receiving basic immunizations or having a sustainable source of income. As Judea Pearl writes in his book "The Art and Science of Cause and Effect" : [Randomized experiments are]... "the only scientifically proven method of testing causal relations from data, and to this day, the one and only causal concept permitted in mainstream statistics."
Credits: Illustrations created using Noto Emoji by Google. Erode, Tanker, and Hind Siliguri tyepfaces used are copyright of Indian Type Foundry. Child and Person icon used to show immunization results are from Font Awesome. Images credited wherever used. ChatGPT for all the coding help.
Sources: These resources were invaluable while writing and designing this article. 1. How randomised trials became big in development economics by The Conversation 2. The Nobel went to economists who changed how we help the poor by VOX 3. How to make dope shit by The Pudding 4. Improving immunisation coverage in rural India by Banerjee et al 5. A multifaceted program causes lasting progress for the very poor by Banerjee et al 6. The Entry of Randomized Assignment into the Social Sciences by Julian C. Jamison. 7. Poor economics by Abhijit Banerjee and Esther Duflo.